

Sim Cases Cliff Notes - January 2018
/
Every month we summarize our simulation cases. No deep dive here, just the top 5 takeaways from each case. This month includes
The Nightmare Neonate and Midgut Volvulus

https://emedicine.medscape.com/article/411249-overview
Malrotation with midgut volvulus shows torsion around the narrow mesenteric stalk.
1. Start with the basics of resuscitating the sick appearing neonate as you know how.
- Check the blood sugar early and often
- 2.5-5 ml/kg D10 bolus for glucose < 45 mg/dL
- If IV access is unattainable and the situation is urgent, an intraosseous (IO) line is a reasonable choice
- Keep thermoneutral under the warmer
- Fluid resuscitate
- 10-20 ml/kg bolus initially and repeat Q 10 min until shock reversal or 60 ml/kg
- Consider smaller boluses (10 ml/kg) if poor cardiac function suspected
- Test, culture and administer antibiotics
- Ampicillin (50 mg/kg) with either cefotaxime (50 mg/kg) or gentamicin (2.5 mg/kg).
2. The septic appearing neonate can be scary - but there is a short list of things that can be wrong with them early in their life. "THE MISFITS" mnemonic is a good differential to start with:
- T Trauma/non-accidental trauma
- H Heart Disease
- E Endocrine (Congenital Adrenal Hyperplasia/Thyroid emergencies)
- M Metabolic disturbances (hypoglycemia, hyponatremia)
- I Inborn Errors of Metabolism
- S Sepsis
- F Formula dilution or Over-concentration
- I Intestinal Catastrophe (midgut volvulus, intususception, necrotizing enterocolitis)
- T Toxins (including home remedies)
- S Seizures
For more details on THE MISFITS mnemonic and differential, check out this great post on EM DOCS
3. Midgut volvulus is a condition in which the intestine has become twisted around the superior mesenteric artery as a result of malrotation of the intestine during fetal development. Malrotation of the intestine occurs when the normal embryologic sequence of bowel development and fixation is interrupted.

- Most common presentation (> 80% of cases) is a newborn infant with bilious vomiting within first month of life, often within the first week of life
- Bilious emesis in a neonate is bad!
- One single-center prospective study found a surgical cause in 38%, including (in descending order of frequency) Hirschsprung disease, bowel atresia, malrotation, meconium ileus, meconium plug, and other inspissation
- In a case series of 52 infants under one year of age, vomiting was the presenting symptom in 93 percent of patients [3]
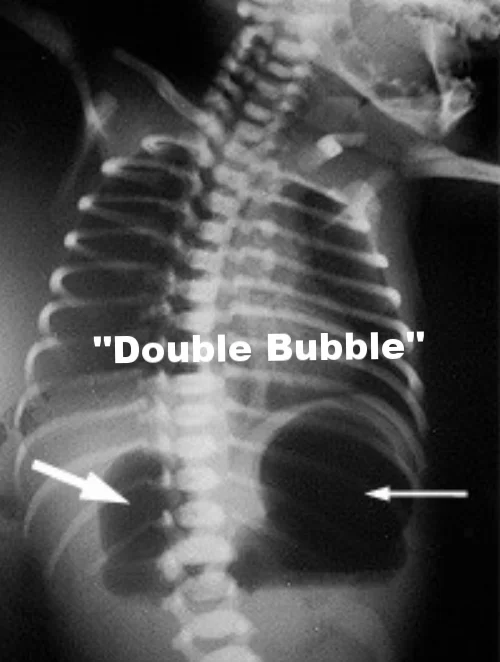
4. Plain films can hint at the diagnosis, but the preferred diagnostic test is an upper GI.
ABDOMINAL XRAY
- May show air-fluid levels
- The plain film on the right shows the "double bubble sign" (due to a disproportonate dilated duodenum)
- The abdominal xray will frequently be read as normal
UPPER GI SERIES
- Sensitivities for detecting malrotation are reported at 93-100%
- An incomplete duodenal obstruction and dilation of the first and second portions are seen, as is the "corkscrew sign"

https://emedicine.medscape.com/article/411249-overview
5. When concerned about volvulus, consult pediatric surgery, place an nasogastric tube and if necrosis or perforation is suspected, administer broad spectrum antibiotics.
- With a high clinical suspicion, don't delay your consult for xrays
- This diagnosis has a high mortality and morbidity
- This is a time dependent diagnosis
- Time is gut!
- Fly your patient to your pediatric surgeon if you need to
References
1. Brousseau T, Sharieff GQ. Newborn emergencies: the first 30 days of life. Ped Clin N Am. Feb 2006; 53:69-84. [Pubmed]
2. McCollough M, Sharieff GQ. Abdominal surgical emergencies in infants and young children. Emerg Med Clin N Am. 2003 Nov;21(4):909-35. [Pubmed]
3. Kim UO, Brousseau D, Konduri G. Evaluation and management of the critically ill neonate in the emergency department. Clin Ped Emerg Med. 2008 Sept;9(3):140-148.[PDF]
4. Godbole P, Stringer MD. Bilious vomiting in the newborn: how often is it pathologic? J Pediatr Surg. 2002;37(6):909-911. [Pubmed]
5. Bonadio WA, Clarkson T, Naus J. The clinical features of children with malrotation of the intestine. Pediatr Emerg Care.
1991;7(6):348-349. [Pubmed]
6. Nehra D, Goldstein AM. Intestinal malrotation: varied clinical presentation from infancy through adulthood. Surgery 2011; 149:386.[Pubmed]
Massive Upper GI Bleeding (GIB)

1. Evaluate for the possibility this could be variceal bleeding early.

- Does the patient have cirrhosis or prior esophageal varices?
- While the cirrhotic patient with massive upper GIB is statistically more likely to have peptic ulcer disease, assume variceal. . . why?
- Variceal GI bleeds are potentially more life threatening
- There is more you can do to stabilize variceal GI bleeding
2. Intubate your patient with a massive upper GIB early.

- A patient with massive GIB is at risk for aspiration and will likely need emergent endoscopy
- The three legged airway/breathing/circulation stool gets thrown off balance with severe bleeding
3. Maximize your medical therapy.

- Crystalloid infusion to achieve a perfusing mean arterial pressure
- Packed red blood cells (give early for shock)
- A restrictive strategy (transfusion only when the hemoglobin level fell below 7 g/dL) has been shown to have reduced mortality when compared to a more liberal transfusion threshold (9g/dL)
- For more on a restrictive transfusion strategy with massive GIB, check out this great podcast from Ken Milne on the Skeptics Guide to Emergency Medicine
- Correct coagulopathy
- Prothrombin complex concentrates
(PCCs) should be first-line - PCCs do not require crossmatch and act more quickly than fresh frozen plasma (FFP) alone
- If PCC's are unavailable, give an initial transfusion of FFP at 10 ml/kg
- For the patient on warfarin, administer Vitamin K at a dose of 5
to 10 mg IV
- Prothrombin complex concentrates
- Somatostatin analogues (Octreotide)
- Octreotide inhibits the secretion of various gastric hormones and can reduce the portal venous blood flow (which could reduce the amount of bleeding in the setting of esophageal varices)
- Somatostatin analogues do not reduce mortality in upper GIB from esophageal varices, but may reduce blood transfusion requirements
- Octreotide 50 mcg IV bolus with 50 mcg/hr gtts
- Proton Pump Inhibitor
- PPI treatment in peptic ulcer bleeding may reduce rebleeding and surgical intervention rates, but has no effect on mortality
- Initial bolus of 80 mg, followed by a continuous infusion of 8 mg/hr for 72 hours (recent studies have shown however non inferiority of intermittent PPI bolus)
- Antibiotics
- Prophylactic antibiotic use in patients with cirrhosis and upper GIB significantly reduces bacterial infections, all-cause mortality, bacterial infection mortality, rebleeding events, and hospitalization length
- Ceftriaxone 1 g IV
4. Activate the chain of survival early. Your interventions may work . . . but if they don't, you need to have the next interventions already in motion.
- Medical therapy alone is unlikely to stop massive upper GI bleeding
- Consult your friendly neighborhood endoscopist early
- Considering activating interventional radiology for a TIPS procedure
- Consider activating surgery (yes, surgery, they still have a role in uncontrollable massive upper GI bleeding)
5. Consider Balloon Tamponade for:

https://en.wikipedia.org/wiki/Balloon_tamponade
- Substantial ongoing upper GI bleeding and delayed endoscopy
- Prolonged transport
- Variceal bleeding that cannot be controlled with endoscopy
References
1. Huang E, Karsan S, Kanwal F, Singh I, Makhani M, Spiegel B. Impact of nasogastric lavage on outcomes in acute GI bleeding. Gastrointest Endosc. 2011;74(5):971-980. [PubMed]
2. Leontiadis G, McIntyre L, Sharma V, Howden C. Proton pump inhibitor treatment for acute peptic ulcer bleeding. Cochrane Database Syst Rev. 2004;(3):CD002094. [PubMed]
3. Sreedharan A, Martin J, Leontiadis G, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2010;(7):CD005415. [PubMed]
4. Bañares R, Albillos A, Rincón D, et al. Endoscopic treatment versus endoscopic plus pharmacologic treatment for acute variceal bleeding: a meta-analysis. Hepatology. 2002;35(3):609-615. [PubMed]
5. Gøtzsche P, Hróbjartsson A. Somatostatin analogues for acute bleeding oesophageal varices. Cochrane Database Syst Rev. 2008;(3):CD000193. [PubMed]
6. Chavez-Tapia N, Barrientos-Gutierrez T, Tellez-Avila F, et al. Meta-analysis: antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding – an updated Cochrane review. Aliment Pharmacol Ther. 2011;34(5):509-518. [PubMed]
7. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11-21. [PubMed]
Written and Posted by Jeffrey A. Holmes, MD








