

Sim Cliff Notes - November 2017
/
Every month we summarize our simulation cases. No deep dive here, just the top 5 takeaways from each case. This month we discussed geriatric trauma and penetrating neck injury.
5 Core concepts for Geriatric Trauma

https://worldwideinterweb.com/elderly-funny-pictures/
1. Elderly patients' diminished physiologic reserves, co-morbidities, and medications make it more difficult for them to recover from traumatic injury.
2. Every component of the primary survey is different in the elderly.

http://www.jems.com/articles/print/volume-39/issue-8/features/dos-and-don-ts-bag-valve-mask-ventilatio.html
Airway – Assess for difficult airway predictors and perform 2 person ventilation
- Direct laryngoscopy is more difficult (impaired neck mobility and mouth opening)
- Bag mask ventilation is more difficult (edentulous, facial wasting, stiff lungs/chest wall)
- Breathing - Provide apneic oxygenation during intubation attempt and be prepared for decreased apneic time to intubate
- Elderly desaturate quickly and tolerate hypoxia poorly (reduced central respiratory drive, weakened respiratory muscles, altered chest wall mechanics)
- Elderly are at increased risk of aspiration (blunted ariway reflexes, swallowing disorders, drug effects, delayed gastric emptying)
- Circulation – Be vigilant for shock and consider reducing sedative doses
- Detection of unrecognized shock may be difficult in older trauma patients
- “Normal blood pressures” may be misleading because of the prevalence of preexisting hypertension (hypotension in elderly trauma patient should be considered SBP less than 110 mm Hg)
- Medications such as beta-blockers may blunt tachycardic response
- Elderly have a reduced “maximal heart rate” (“tachycardia” should be considered a heart rate greater than 90)
- Age – related cardiovascular changes, pre-existing disease, and drug interactions enhance hypotensive response to induction and reduced doses (20-30%) of sedatives and hypnotics should be considered
- Detection of unrecognized shock may be difficult in older trauma patients

http://slideplayer.com/slide/3846013/
- Disability – Even minor mechanisms can cause intracranial hemorrhage and cervical spine fractures
- Age related cerebral atrophy stresses and stretches bridging veins, leading to subdural hematomas with minimal shearing stress
- Age related atrophy leads to cerebral contusions due to coup and contracoup impact
- Osteoporosis and other factors make cervical spine fractures 2x as common in elderly, almost half from ground level fall
3. Always consider if a decompensated medical illness (e.g., infection, myocardial infarction) may have precipitated or be exacerbated by their trauma. Have a low threshold for additional testing (eg. ECG).

https://lifeinthefastlane.com/ecg-library/basics/complete-heart-block/
4. Elder abuse is very under recognized and under reported. Be vigilant for subtle signs of elder abuse and ask your patient (Click here for our recent post on elder abuse)
- The U.S. Department of Justice estimates that 1 in 9 Americans over 60 years old will experience abuse, neglect exploitation this year
- It is estimated that only 1 in 14 elders will report elder abuse
- Victim risk factors include Age > 75, low income, social isolation, minority , financial dependence on caregiver, cognitive impairment
5. The decision to discharge an elderly patient needs to be made with a number of caveats in mind.
- The need for arm slings, crutches, canes and walkers all contribute to gait instability and could lead to a fall without proper social support for patient
- Lower extremity orthopedic injuries confer a particularly high risk for elderly patients, andadmission should be strongly considered
- Any patient who has gait instability, generalized weakness, profound fatigue after their traumatic event, or a recent history of recurrent falls is a poor candidate for discharge
References
1. Brown JB, Gestring ML, Forsythe RM, et al. Systolic blood pressure criteria in the National Trauma Triage Protocol for geriatric trauma: 110 is the new 90. J Trauma Acute Care Surg 2015;78: 352-359.
2. Pontoppidan H, Geffin B, Lowenstein E. Acute respiratory failure in the adult. N Engl J Med 1972; 287(14):690-8.
3. Milzman DP, Rothenhaus TC. Resuscitation of the geriatric patient. Emerge Med Clin North Am 1996: 14(1):233-44
4. Wang H, Coppola M, Robinson RD, et a. Geriatric trauma patients with cervical spine fracture due to ground level fall: Five years experience in a level one trauma center. J Clin Med Res 2013; 5:75-83.
5, McGwin G, Jr., Sims RV, Pulley L, Rosemen JM. Relations among chronic medical conditions, medications, and automobile crashes in the elderly: a population-based case-control study. Am J Epidemiol 2000: 152(5):424-31.
6. McGwin G, Jr., Maclennan PA, Fife JB, Davis GG, Rue LW, 3rd. Preexisting conditions and mortality in older trauma patients. J Trauma 2004; 56 (6):1291-6.
7. American Geriatric Society, British Geriatrics society, and American Academy of Orthopaedic Surgons Panel on falls Prevention. Guidelines for the prevention of falls in older person. J AM Geriatr Soc 2001; 49 (5):664-72.
8. Acierno R, Et al. Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: the National Elder Mistreatemnt study. Am J Public Heath. 2010; 100 (2): 2929-297.
5 step approach to Penetrating Neck Injury (PNI)
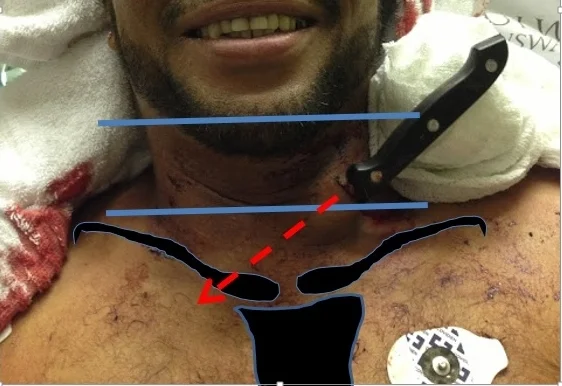
1. It pays to know your anatomy. . . ask yourself these questions:
Does it violate the platysma?
- The platysma is the anatomic landmark that defines PNI and requires you to do more than simple wound management.
- The platysma is a very thin muscle invested in the subcutaneous fascia (it can be very difficult to identify).
- Gently spread (no probing) the wound edges apart to evaluate if the wound has violated the platysma.

http://aclandanatomy.com/multimediaplayer.aspx?multimediaid=10528465
Is the wound in the anterior or posterior triangle?
- ANTERIOR TRIANGLE: Contains more critical structures (Carotid artery, Internal jugular, Vagus nerve, Trachea), more surgically accessible
- POSTERIOR TRIANGLE: Considered a lower risk area (although tragectory of PNI can course back into anterior triangle), contains cervical cord/spine



http://m.trauma.utoronto.ca/protocols/penetrating_neck_trauma.html
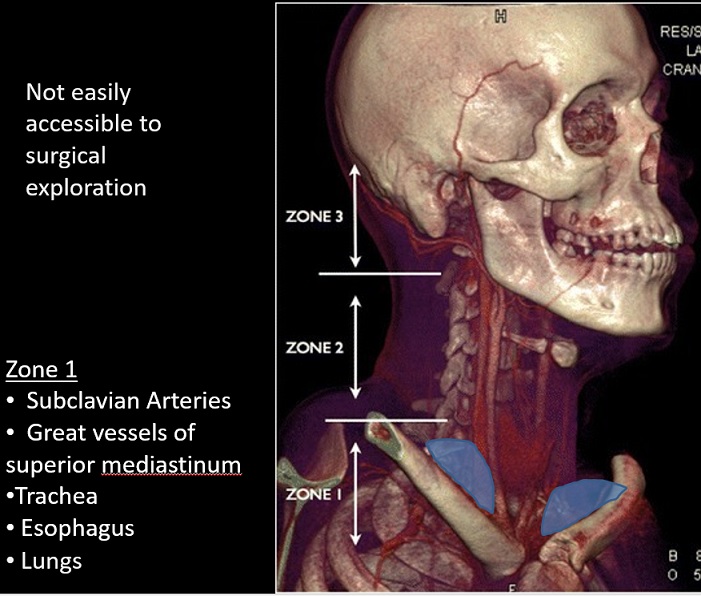
What zone is it in?
- Identifying the zone helps anticipate the anatomy that could potentially be injured
Zone designation carries implications for management and prognosis
However, there are problems with the "zone system"
- Refers only to the location of the wound, not the tract of the penetrating object
- Injury to one zone can extend into different zones
- Past algorithms dictated workup/managment based on zone - less so today
- Current PNI diagnosis/treatment algorithms focus on the exam and CTA


2. Perform a targeted history and physical exam, looking for hard signs that mean an immediate trip to the OR (before or after airway management).
- Physical Exam
- Is there an expanding hematoma?
- Bubbling wound?
- Crepitus?
- Stridor?
- Vascular or neurologic deficit?
- Bruit/thrill?
- History
- Are they hoarse?
- Do they have dysphagia?
- Was there pulsatile bleeding prehospital?
- Hemoptysis?
3. Patients with PNI require frequent re-evaluation of their airway - sick trauma patients live or die from problems with their primary survey.

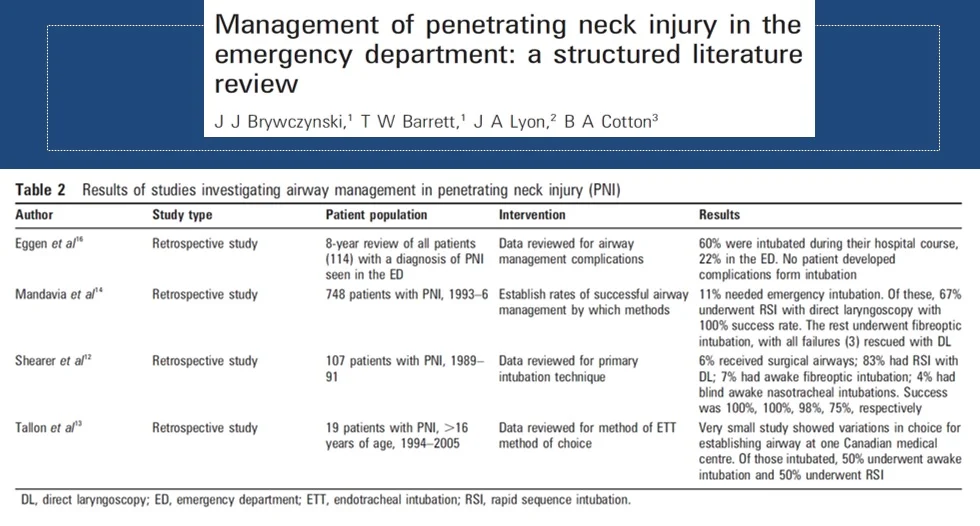
4. If you have to intubate, rapid sequence intubation with video laryngoscopy is probably the best method.
- A large meta-analysis of PNI by Brywczynski et al. helps inform our choice of intubation method (see table 2 below)
- Rapid sequence intubation with direct laryngoscopy has been shown to be successful and effective
- Concern that complete muscle relaxation in a distorted airway could lead to obstruction are unlikely
- Surgical airways are rare (6%)
- Multiple methods have proven successful, however failure rates are higher with nasotracheal intubation
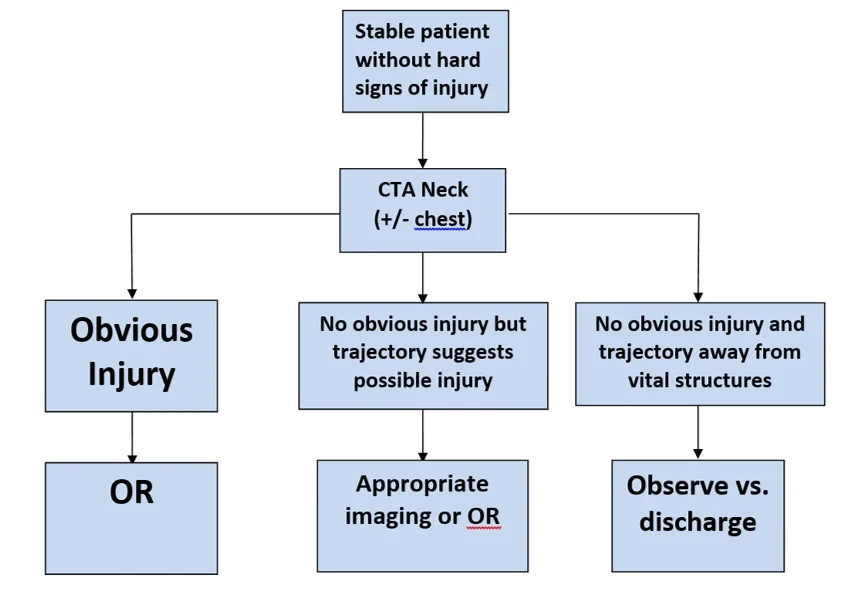
5. The current paradigm for PNI that is stable without hard findings includes CTA of the neck (+/- chest) and selective operation.

References
1. Brywczynski JJ1, Barrett TW, Lyon JA, Cotton BA. Management of penetrating neck injury in the emergency department: a structured literature review. Emerg Med J. 2008 Nov;25(11):711-5. doi: 10.1136/emj.2008.058792.
2. Inaba K. et al. Evaluation of multidetector computed tomography for penetrating neck injury: a prospective multicenter study. Emerg Med J. 2008 Nov;25(11):711-5. doi: 10.1136/emj.2008.058792.
3. Tisherman AT, Bokhari F, Collier B, et al. Clinical practice guidelines: penetrating neck trauma. J Trauma. 2008;64(5):1392-1405.
4. Schaider J, Bailitz J. Neck trauma: don’t put your neck on the line. Emergency Medicine Practice. 2003;5(7):1-28.








