

Simulation Cases Cliff's Notes - November 2019
/
Every month we summarize our simulation cases. No deep dive here, just the top 5 takeaways from our high fidelity simulation case.

5 step approach to Massive Hemoptysis
1. RECOGNIZE MASSIVE HEMOPTYSIS
The majority of hemoptyis seen in the emergency department is minor (i.e. from an etiology such as bronchitis) and does not need intervention
The textbook definition for massive hemoptysis is 600 cc or more in 24 hours
The more practical definition of massive hemoptysis is independent of volume - if there is impaired gas exchange, airway obstruction, or hemodynamic stability, it’s time to intervene!
2. ENSURE RESPIRATORY AND CONTACT PRECAUTIONS
Infectious disease (especially tuberculosis) is a major cause of massive hemoptysis
Make sure you protect yourself with eyewear, an impervious gown, gloves and N95 mask
If possible, place the patient in a negative pressure room until tuberculosis can be ruled out

3. UNDERSTAND MASSIVE HEMOPTYSIS IS AN AIRWAY PROBLEM
Although hemoptysis is from bleeding, the life threat is asphyxiation (not hemorrhagic shock)
It only takes 150 - 200 cc of blood to fill your tracheobronchial tree and obstruct gas exchange
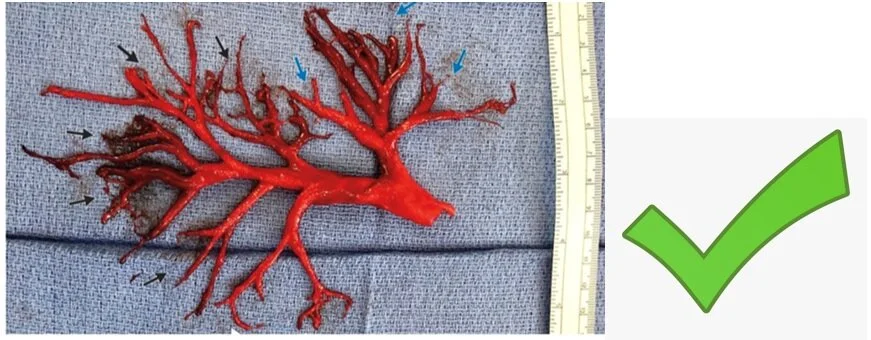
Blood clot cast of a tracheobronchial segment

3. PROTECT THE AIRWAY

Large diameter Ducanto Catheter compared to a traditional suction catheter
Have your airway backup vetted and ready as blood is the enemy to fiberoptics and video laryngoscopy
Be ready for large volume suction with two yankeuers (or better yet, use a Ducanto catheter)
Use the largest endotracheal tube (ETT) you can (8.5 or greater) to facilitate suctioning and bronchoscopy
Lateralize (and localize) the bleeding on chest xray (or CTPA if stable and XR was inconclusive)
Selectively perform main stem intubation of the nonaffected side to prevent filling of the contralateral tracheobronchial tree
Right main stem intubation is easier given the angle of that bronchus
Intubating the left main stem is more challenging.
Bair et al. published a successful technique for main stem intubation by rotating the ETT
Gottlieb et al. published a successful technique for main stem intubation using a bougie
4. CORRECT ANY COAGULOPATHY/PLATELET DYSFUNCTION
If available, provide a reversal agent for direct oral anticoagulants (check out our guideline for the management of bleeding on Dabigatran and the management of bleeding on Rivaroxaban or Apixaban)
Protein Complex Concentrates for Warfarin
DDAVP for platelet dysfunction (classically in uremic patients)
Tranexamic acid 1 gram IV over 10 minutes
5. IDENTIFY THE SITE OF BLEEDING AND MOBILIZE THE TROOPS

Treating massive hemoptysis is a team sport
Mobilize your resources early for source control
Consult pulmonary for therapeutic bronchoscopy, insertion of an endobronchial blocker
Consult interventional radiology for bronchial artery embolization
95% of bleeding in massive hemoptysis is from a bronchial artery
Consult cardiothoracic surgery for possible resection
Other FOAMed Reviews on Massive Hemoptysis
Written by Jeffrey A. Holmes, MD
Peer Reviewed by Jason Hine, MD
References
1. Brown CA and Raja AS. Chapter 24. Hemoptysis. In: Marx JA et al. eds. Rosen’s Emergency Medicine, 8e. Philadelphia: Elsevier Saunders; 2014.
2. Ibrahim WH. Massive haemoptysis: the definition should be revised. Eur Respir J. 2008 Oct;32:1131-2. [Pubmed]
3. Sakkour A and Susanto I. Airway management in massive hemoptysis. Emergency Med & Crit Care Rev 2006.[Pdf]
4. Swanson, KL, et al. Bronchial artery embolization: experience with 54 patients Chest 2002; 121:789.[Pubmed]
5. Bair AE et al. An evaluation of a blind rotational technique for selective mainestem intubation. Acad Emerg Med. 2004 Oct; 11 (10) 1105-7. [Pubmed]
6. Gottlieb, M et al. Utilization of a gum elastic bougie to facilitate single lung intubation. Am J Emerg Med. 2016 Dec; 34 (12): 2408-2410.[Pubmed]








