


Digital Nerve Block
Anatomy:
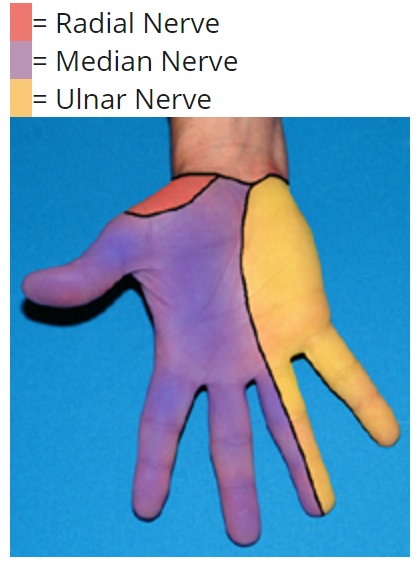
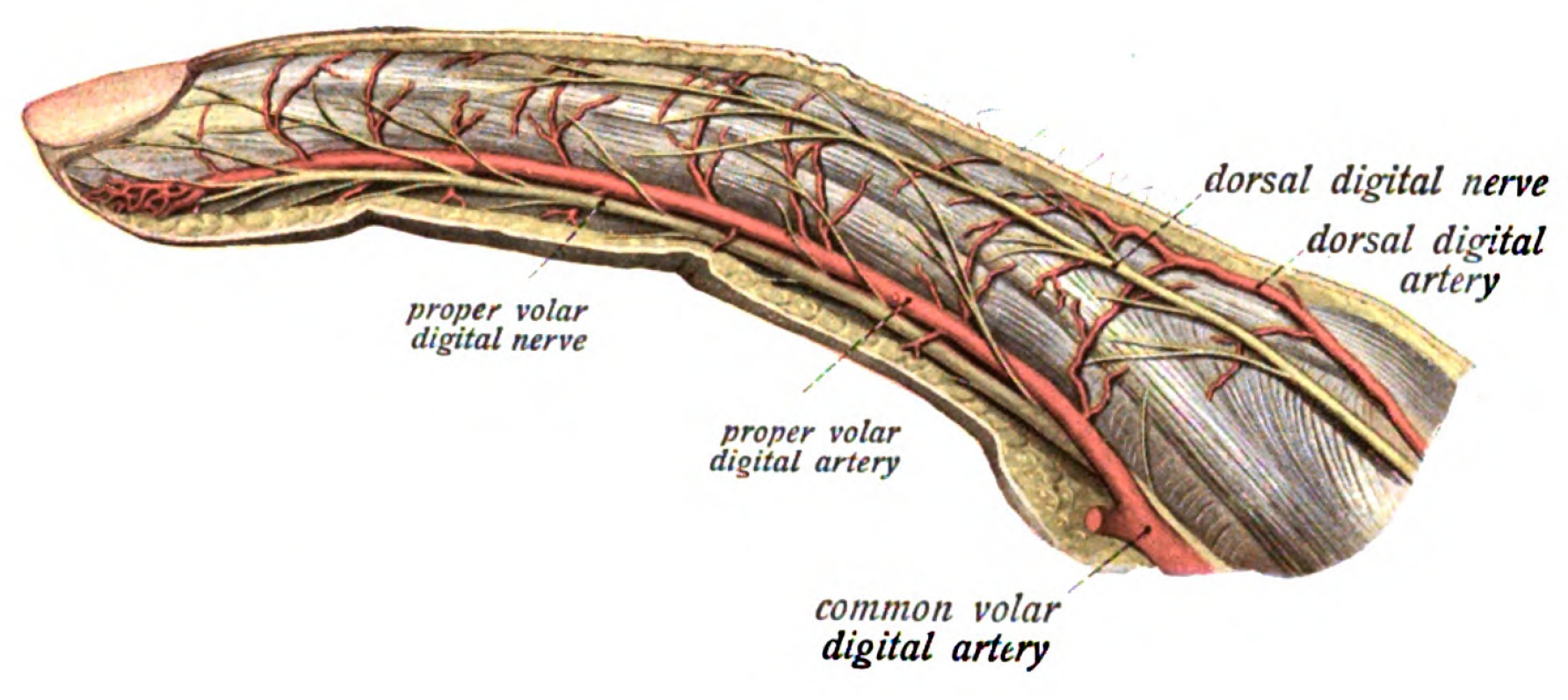
- The common digital nerves are derived from the median and ulnar nerves and divide in the distal palm into paired palmar branches. The nerves travel on either side of the flexor tendon sheath of each finger and innervate the lateral and palmar aspect of each finger. The smaller dorsal digital nerves, derived from the radial and ulnar nerves, run on the dorsal lateral aspect of each finger and supply sensation to the back of the finger.
Distribution of anesthesia:
- The digital nerve block provides anesthesia to the entire digit.
Technique:

- The surgical field should be prepared as close as possible to the metacarpophalangeal joint. While the procedure can be performed from either the volar or dorsal aspects of the digit; the later is less painful. Raise a wheal of anesthesia in the subcutaneous space and direct the needle palmar on both the medial and lateral aspect of the first phalange. To insure inadvertent vessel puncture, aspirate as you insert the needle. Apply one to two milliliters of anesthesia slowly as you are withdrawing the needle. Allow five to ten minutes for full anesthesia with lidocaine and fifteen to twenty minutes with bupivacaine. If this procedure does not provide complete anesthesia, more anesthetic may be needed by either reapplication of the digital nerve block or performing a transthecal digital nerve block.

Transthecal Approach
- The transthecal approach utilizes the flexor tendon sheath to apply anesthetic to the digital nerves. This procedure can be performed in addition to or as an alternative to a digital nerve block.
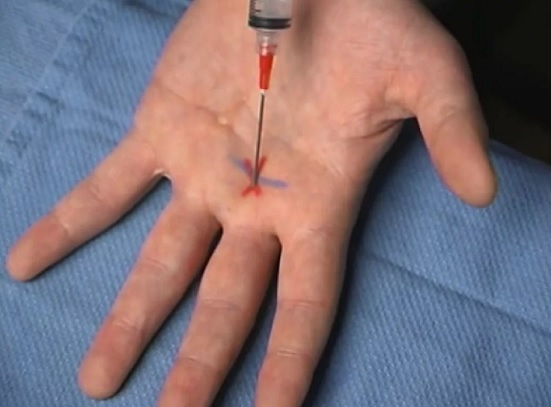
- Identify the flexor tendon sheath of the digit to be blocked at the palmar aspect of the hand. Have the patient flex the finger to be blocked if possible. At the level of the distal palmar crease, puncture the skin at a forty-five degree angle until the pop of the flexor tendon sheath is felt. If this "pop" is not felt, continue to insert the needle, aspirating as you inject, until the needle contacts bone. Withdraw the needle two to five millimeters and inject 2 to 3 ml of anesthesia. When the needle is in the flexor tendon sheath, the anesthesia should flow easily. As before, allow five to ten minutes for full anesthesia with lidocaine or fifteen to twenty minutes with bupivacaine.
Pitfalls:
- Not performing a transthecal block with a failed dorsal digital block.
- Intraneural injection will cause significant pain, therefore withdraw the needle a few millimeters and continue injecting the anesthetic.
Intrathecal Digital Nerve Block
Ulnar Nerve Block

Anatomy:
Identify the flexor carpi ulnaris and ulnar artery by having the have the patient deviate their hand in an ulnar direction at the wrist (giving the thumbs up). The flexor carpi ulnaris is the most medial (ulnar) tendon. The ulnar artery can be palpated just medial and dorsal to the tendon. The nerve lies between the artery and the flexor carpi ulnaris tendon.
Distribution of anesthesia:
This procedure provides anesthesia to the entire fifth digit, half of the fourth digit and the medial aspect of the hand and wrist

BLUE= flexor carpi ulnaris; large red dot = injection point for ulnar nerve; small red dots = infiltrative area to anesthetize cutaneous branches of ulnar nerve
Technique:
The surgical field should be prepared just proximal (1-2 cm) to the most distal wrist crease. Raise a wheal of anesthetic in the subcutaneous space and insert the needle under the flexor carpi ulnaris one centimeter just palmar to the ulnar styloid. If blood is aspirated, withdraw the needle a few millimeters and aspirate again, the nerve is more superficial from the injection point. Inject approximately 5 to 7 milliliters of anesthetic. To block the cutaneous branches of the ulnar nerve, inject 3 to 5 milliliters of anesthetic just above the tendon of the flexor carpi ulnaris.
Pitfalls:
- If bone is struck withdraw the needle and direct it more palmar.
- Intraneural injection will cause significant pain, therefore withdraw the needle a few millimeters and continue injecting the anesthetic.
Ultrasound Guided Ulnar Nerve Block
Median Nerve Block
Anatomy:
- Identify the flexor carpi radialis and the palmaris longus tendons at the palmar aspect of the wrist. The palmaris longus, if present, is usually the more prominent of the two tendons and can be identified by having the patient flex at the wrist. To help identify the flexor carpi radialis, have the patient flex and abduct the wrist. The median nerve is lateral (radial) to the palmaris longus tendon and between the palmaris longus and the flexor carpi radialis.
Distribution of Anesthesia:
- The median nerve provides sensory to the lateral three and a half digits except the dorsal aspect of the thumb, and the corresponding area of the palm.

BLUE = Palmaris longus tendon; red = median nerve
Technique:
- The surgical field should be prepared across the entire volar surface of the wrist at the proximal palmar crease. Raise a wheal of anesthetic in a subcutaneous space and insert the needle until it pierces the deep fascia. If the "pop" of the deep fascia can not be felt, continue to insert the needle until it contacts the bone. Withdraw the needle 2 to 5 millimeters and inject 5 to 7 milliliters of anesthetic. A fan like technique is recommended to ensure complete anesthesia of the median nerve. This can be accomplished by reinserting the needle in the same position approximately 30 degrees medial and 30 degrees lateral and injecting 2 to 5 additional milliliters of anesthetic. The palmar branch of the medial nerve is quite superficial and can be blocked by withdrawing the needle to the subcutaneous space and injecting 3 to 5 milliliters of anesthesia.
Pitfalls:
Avoid injecting too distal within the carpal tunnel which may exacerbate any carpal tunnel syndrome.
Intraneural injection will cause significant pain, therefore withdraw the needle a few millimeters and continue injecting the anesthetic.
Ultrasound Guided Median Nerve Block
Radial Nerve Block

Anatomy:
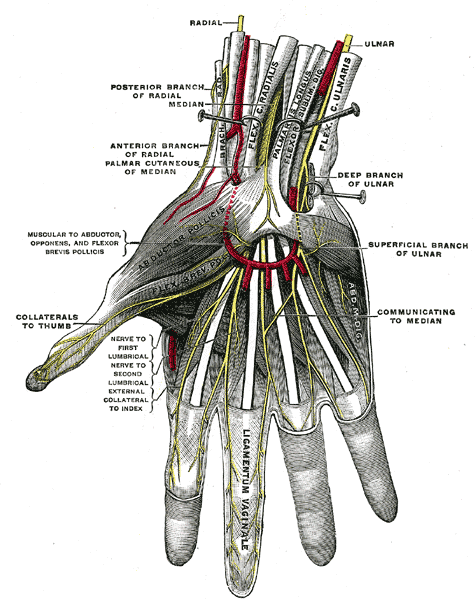
Locate the radial styloid at the proximal portion of the anatomic snuff box. The anatomic snuff box is just distal to the radial styloid and formed by the extensor tendon of the palmaris brevis and longus. The superficial branch of the radial nerve runs just above the styloid process of the radius. It gives off digital branches to the dorsum of the thumb, index finger and lateral half of the middle finger. Several branches run over the anatomic snuff box. The nerve divides into two major branches about two finger breadths proximal to the distal wrist crease (or anatomical snuff box).
Distribution of anesthesia:
The radial nerve provides sensory innervation to the dorsal lateral half of the hand and the dorsal aspect of the thumb. The radial nerve provides no motor innervation to the intrinsic muscles of the hand however; it does provide innervation for all of the extensor muscles in the posterior forearm.
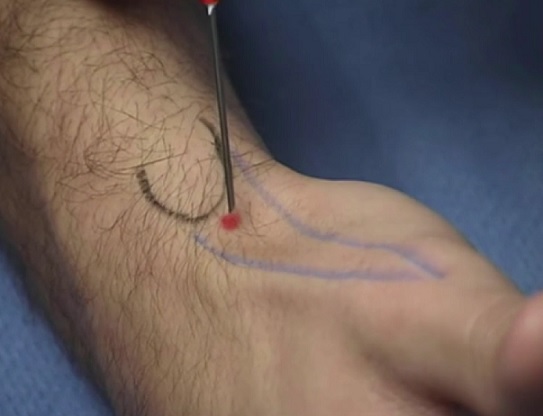
blue = extensor tendons of palmaris longus and brevis; black = radial styloid; red = injection point for radial nerve block
Technique:
The surgical field should be prepared across the entire dorsal surface of the wrist, including the radial styloid and the anatomic snuff box. Raise a wheal of anesthesia in the subcutaneous space and inject 5 to 7 milliliters of anesthetic just above the radial styloid, aiming the needle first medially and then laterally.
Alternative method:
- Using the non-injecting hand, straddle the anatomic snuffbox with the index and middle fingers and press them firmly against the radius. Slowly inject the anesthetic which will spread across the path of the nerve.
Pitfalls:
The distribution of the radial nerve is less predictable; therefore, a generous amount of anesthesia should be injected. Intraneural injection will cause significant, therefore withdraw the needle a few millimeters and continue injecting the anesthetic.
Ultrasound Guided Radial Nerve Block
Written by Douglas Dillon, MD
Ultrasound videos produced by Peter Croft, MD
Edited and posted by Jeffrey A. Holmes, MD








